
Radiofrequency ablation (RFA) can be used to treat some thyroid cancers — but only in very specific cases. It’s best suited for small, low-risk thyroid cancers (especially papillary thyroid cancers that haven’t spread), and for people who can’t or don’t want to have surgery.
If the cancer is small, contained inside the thyroid, hasn’t spread to lymph nodes, and you’re being treated at an experienced center, RFA can be an effective, minimally invasive alternative. But for most thyroid cancers, surgery is still the gold standard treatment.
 What Is Thyroid RFA?
What Is Thyroid RFA?
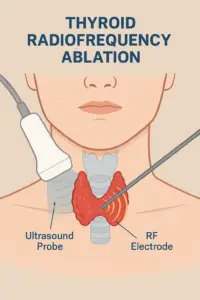
RFA is a minimally invasive procedure that uses heat (radiofrequency energy) to destroy abnormal thyroid tissue. It’s done through a thin needle guided by ultrasound — no large incision, no general anesthesia, and usually minimal downtime.
It’s already well-established for treating benign thyroid nodules (non-cancerous growths that cause swelling, pressure, or cosmetic issues). But its use for thyroid cancer is newer and still evolving.
When Can RFA Be Used for Thyroid Cancer?
Doctors are exploring RFA as an option for select thyroid cancer cases. Here’s when it may be considered:
1. Very Small, Low-Risk Thyroid Cancers
RFA may be used to treat small papillary thyroid cancers — usually less than 1 cm (microcarcinomas) or sometimes up to 2 cm if the tumor is completely inside the thyroid and hasn’t spread.
-
Studies show RFA can remove these small tumors effectively with very low recurrence rates.
-
It’s typically considered when the cancer is found early and is limited to one spot.
2. Recurrent Thyroid Cancer
If thyroid cancer comes back in the neck lymph nodes after surgery, RFA can sometimes target those small areas instead of doing another major operation — especially if the repeat surgery would be high-risk.
3. When Surgery Isn’t an Option
For patients who have health issues that make surgery unsafe, or who simply don’t want surgery, RFA can be a reasonable alternative if the tumor meets certain safety criteria.
Who Is a Good Candidate for Thyroid RFA?
A good candidate for RFA usually meets all of these conditions:
-
✅ The tumor is small — ideally under 1 cm (some centers may treat up to 2 cm).
-
✅ The cancer hasn’t spread beyond the thyroid (no lymph nodes or distant metastasis).
-
✅ No invasion into nearby structures like the trachea, esophagus, or vocal cord nerves.
-
✅ The tumor is visible and accessible on ultrasound for precise targeting.
-
✅ You either cannot have surgery for medical reasons or prefer not to have it.
-
✅ You’re treated by an experienced RFA team (interventional radiologist or endocrine surgeon trained in thyroid ablation).
If you fit that profile, RFA could be an appropriate and safe treatment option.
Who Is Not a Good Candidate?
RFA is not recommended for everyone. You’re probably not a candidate if:
-
❌ The tumor is larger than 2 cm or there are multiple tumors.
-
❌ The cancer has spread to lymph nodes or other parts of the body.
-
❌ The tumor is too close to critical structures (like the vocal cord nerve or major blood vessels).
-
❌ You have aggressive cancer types or features suggesting fast growth.
-
❌ You’re looking for a one-time cure without long-term follow-up.
-
❌ You’re being treated in a center without RFA experience.
If any of these apply, surgery is usually the safer and more effective route.
What Are the Benefits of RFA?
When performed in the right setting and by the right team, RFA has several benefits:
-
Minimally invasive: No large incision or general anesthesia.
-
Quick recovery: Usually done as an outpatient procedure.
-
Cosmetic advantage: No neck scar.
-
Less risk of complications compared to surgery (like hypocalcemia or permanent voice changes).
-
Preserves thyroid function — most patients still have normal thyroid hormone levels afterward.
For some patients, that means keeping their thyroid, avoiding lifelong thyroid medication, and going home the same day.
What Are the Risks or Limitations?
RFA is generally safe, but it’s not risk-free. Potential issues include:
-
Incomplete treatment: Some cancer cells may remain, requiring repeat treatment or surgery later.
-
Voice changes: If the heat spreads too close to the recurrent laryngeal nerve (rare in experienced hands).
-
Swelling or temporary pain: Common right after the procedure.
-
Unknown long-term data: RFA hasn’t been around as long as surgery for cancer, so we’re still learning how outcomes compare over 10–20 years.
Most importantly, RFA requires regular follow-up. Even after a successful ablation, patients need routine ultrasounds (and sometimes biopsies) to ensure the cancer hasn’t returned.
What Do Major Medical Guidelines Say?
The American Thyroid Association (ATA) currently recognizes RFA as a potential option only in select, low-risk cases — not as a replacement for surgery. More research is underway, and early results are very promising, but long-term data are still being collected.
In many countries (like South Korea, Italy, and China), RFA for small thyroid cancers has already become a mainstream option due to strong early outcomes and patient satisfaction.
What to Ask Your Doctor
If you’re considering RFA, here are a few smart questions to bring up:
-
Am I a candidate for RFA based on my tumor size and location?
-
How much experience does your team have with thyroid RFA?
-
What are the chances I’ll need a second treatment?
-
How will we monitor for recurrence afterward?
-
What are the risks compared to surgery in my case?
-
What are the costs and insurance coverage for RFA?
The Bottom Line
RFA can be a safe and effective alternative to surgery for certain patients with small, low-risk thyroid cancers — especially those who can’t or don’t want surgery. But it’s not suitable for everyone.
If you’re considering this option, get evaluated by a multidisciplinary team (endocrinologist, surgeon, interventional radiologist) experienced in thyroid cancer care. They’ll help you weigh the pros and cons based on your specific situation.
For now, think of RFA as a minimally invasive tool — not a complete replacement for surgery, but a great alternative for the right patient, in the right hands.
References:
-
American Thyroid Association (ATA) – Thyroid Radiofrequency Ablation Studies, 2024
-
Frontiers in Endocrinology – RFA for Low-Risk Papillary Thyroid Microcarcinoma
-
UCLA Health – Thyroid RFA Program Overview
-
ScienceDirect – Guidelines for Thyroid RFA in Malignant Nodules
Ahmet Ergin MD
Diabetes, Thyroid & Hormone Center Of The Treasure Coast
